

What is cellular senescence: causes, effects, and research
TL;DR:
- Cellular senescence involves an irreversible halt in cell division caused by stress and contributes to aging and disease. Nearly all senescence triggers activate p16 and p21 pathways, leading to a metabolically active but non-dividing cell that secretes inflammatory signals. Current research focuses on therapies to selectively eliminate these cells, but challenges include marker specificity, tissue effects, and biological variability.
Cellular senescence is defined as the permanent arrest of cell division in a living cell, triggered by stressors such as DNA damage, oxidative stress, or telomere shortening. The cell stops replicating but remains metabolically active, secreting a cocktail of pro-inflammatory signals known as the Senescence-Associated Secretory Phenotype, or SASP. Key molecular markers include the cyclin-dependent kinase inhibitors p16 and p21, alongside senescence-associated β-galactosidase as a standard laboratory indicator. The ICCARP consensus recognises senescence as both a protective mechanism and a driver of age-related disease, making it one of the most consequential processes in human biology.
What is cellular senescence and what triggers it?
Cellular senescence is an irreversible cell cycle arrest that occurs when a cell encounters a stress it cannot resolve by dividing. The most studied trigger is replicative exhaustion: human fetal fibroblasts divide approximately 50 times before reaching the Hayflick limit, at which point their telomeres become critically short and division halts permanently. This limit is not a flaw in biology. It is a safeguard against damaged cells proliferating unchecked.
Beyond telomere shortening, senescence can be induced by oncogene activation, persistent DNA double-strand breaks, and chronic oxidative stress. Each of these triggers converges on two core regulatory pathways governed by p16 and p21. These proteins inhibit cyclin-dependent kinases, locking the cell in a non-dividing state. The result is a cell that is alive, active, and secreting signals, but permanently removed from the cell cycle.
Senescence differs from two related states that are often confused with it. Quiescence is a reversible pause in division; the cell can re-enter the cycle when conditions improve. Terminal differentiation is a permanent exit from division, but the cell takes on a specialised function, such as a muscle fibre or neuron. Senescence is neither: the cell retains no specialised function and cannot resume dividing.
Pro Tip: When reading research papers on senescence, check which markers were used to confirm the senescent state. SA-β-gal alone is insufficient; robust studies combine it with p16 or p21 expression and SASP profiling.
The SASP secretion is what makes senescent cells biologically potent beyond their own fate. SASP components include interleukins, matrix metalloproteinases, and growth factors that alter the behaviour of neighbouring cells. This paracrine signalling is central to both the beneficial and harmful roles of senescence.
What are the types of cellular senescence?
Senescence occurs in two distinct forms, and conflating them leads to a distorted picture of the biology.
-
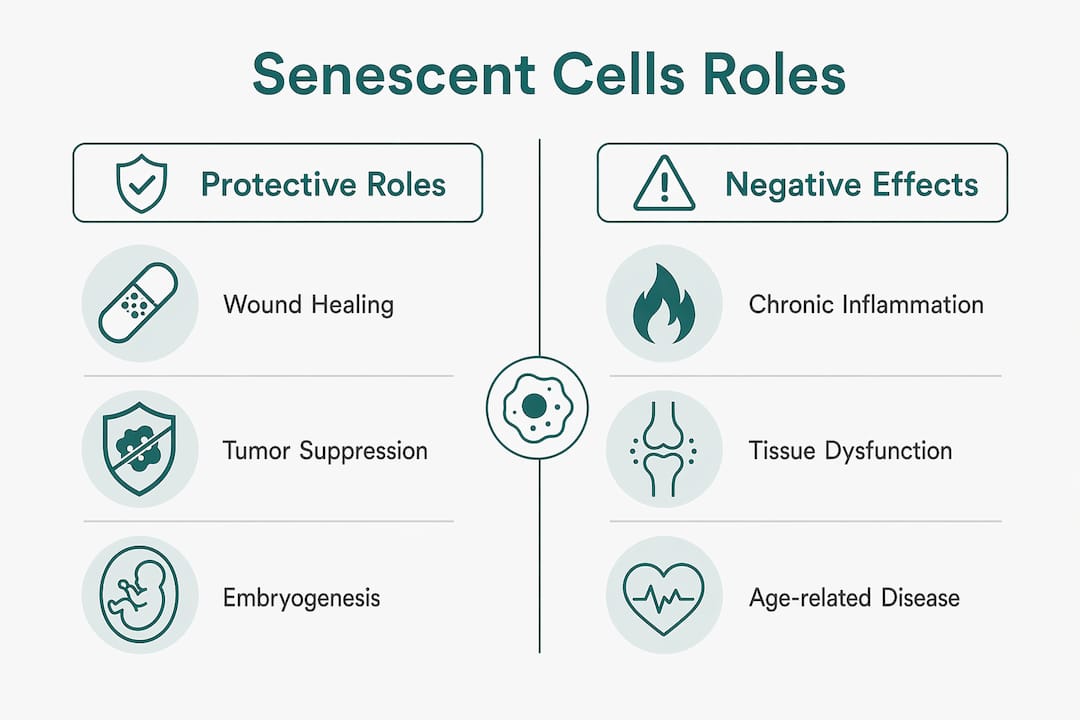
Acute senescence is transient and physiological. The immune system recognises and clears these cells efficiently, maintaining tissue health. Acute senescence plays documented roles in wound healing, tissue remodelling, and embryogenesis. In a healing wound, for example, senescent fibroblasts secrete PDGF-AA, a growth factor that recruits myofibroblasts to close the wound. Once the repair is complete, immune clearance removes the senescent cells.
-
Chronic senescence is persistent accumulation that occurs when immune clearance fails or is overwhelmed. These cells remain in tissues for extended periods, continuously secreting SASP factors. This sustained inflammatory signalling disrupts tissue architecture and contributes to the pathological consequences discussed below.
-
Oncogene-induced senescence (OIS) is a specific subtype triggered when a proto-oncogene mutates and fires inappropriately. The cell arrests before it can become cancerous. This is one of the body’s primary tumour-suppression mechanisms.
The distinction between acute and chronic senescence carries a direct practical implication. Indiscriminate removal of senescent cells can impair wound healing and embryonic development, processes that depend on acute senescence being present at the right time and place.
“Cellular senescence evolved as a key tumour-suppressor mechanism, but it can paradoxically promote tumour progression in already transformed cells. The same SASP that recruits immune cells to clear a pre-cancerous lesion can, in a different context, fuel the growth of an established tumour.”
This dual role is why researchers describe senescence as a double-edged sword. The biology does not permit a simple verdict of “good” or “bad.”
What negative effects are linked to cellular senescence?
Chronic accumulation of senescent cells is associated with a broad range of age-related diseases, including cancer, neurodegeneration, pulmonary fibrosis, and metabolic syndromes. The mechanism is largely SASP-driven: persistent low-grade inflammation degrades the extracellular matrix, impairs stem cell function, and creates a tissue environment that favours disease progression.
Senescent cells also resist apoptosis, the normal programmed cell death pathway. This resistance is not accidental. Anti-apoptotic pathways are upregulated in senescent cells, likely as a mechanism to prevent premature death during acute, beneficial senescence. In chronic senescence, the same resistance becomes a liability, allowing dysfunctional cells to persist and accumulate over decades.
| Disease area | Senescence mechanism |
|---|---|
| Pulmonary fibrosis | Senescent alveolar cells secrete TGF-β, driving fibrotic remodelling |
| Neurodegeneration | SASP promotes neuroinflammation and impairs neuronal repair |
| Metabolic dysfunction | Senescent adipose cells disrupt insulin signalling via IL-6 and TNF-α |
| Cancer progression | SASP in transformed tissue can accelerate tumour growth and metastasis |
A further complication is the heterogeneity of senescent cells. Different triggers produce different senescent phenotypes, and the SASP composition varies considerably by cell type, tissue context, and the nature of the original stress. This makes universal clinical identification difficult. SA-β-gal remains the most widely used marker, but it is not specific to senescence and can appear in other cellular states.
Pro Tip: If you are following senolytic research, pay attention to which cell types and tissues were studied. A therapy that clears senescent cells in adipose tissue may have very different effects in lung or brain tissue.
Ageing is increasingly understood not simply as the accumulation of senescent cells, but as a failure of immune clearance to keep pace with their generation. This reframing shifts focus from the senescent cell itself to the immune environment that allows it to persist.
How is research progressing on targeting senescent cells?
Senolytic therapies aim to selectively eliminate senescent cells by exploiting their dependence on anti-apoptotic survival pathways. The rationale is straightforward: if senescent cells survive by upregulating BCL-2 family proteins, then inhibiting those proteins should trigger their death while leaving normal cells unaffected. Early experimental work in animal models showed reductions in age-related pathology following senolytic treatment.
The clinical translation, however, faces significant obstacles:
- Marker specificity. No non-invasive biomarker currently identifies senescent cells with sufficient precision in living humans. Senolytic therapies remain experimental and are limited by this diagnostic gap.
- Tissue context. Clearing senescent cells in one tissue may have unintended consequences in another, particularly where acute senescence is ongoing.
- Timing. Removing senescent cells at the wrong stage of a wound-healing or immune response could impair recovery rather than support it.
- Heterogeneity. Because senescent cells vary so widely in phenotype, a single senolytic agent is unlikely to address all pathological senescence across different tissues.
Research groups are also exploring senomorphic approaches, which aim to suppress SASP without killing the senescent cell. This preserves any beneficial functions while reducing the inflammatory burden. Both strategies are active areas of investigation, and neither has yet produced a clinically approved therapy for senescence-related ageing.
The science of biological ageing is advancing rapidly, and senescence research sits at its centre. The field is moving from descriptive biology toward mechanistic intervention, but the complexity of the system demands caution.
What examples illustrate cellular senescence in human biology?
Concrete examples make the abstract mechanisms tangible.
The Hayflick limit is the clearest cellular senescence example in human biology. Human fetal lung fibroblasts in culture divide roughly 50 times before entering permanent arrest. This is replicative senescence in its purest form, driven by progressive telomere shortening with each division cycle.
In healthy lung tissue, senescent cells are rare. About 0.27% of alveolar type 2 cells in aged human lung tissue are senescent. This low prevalence is significant. Ageing does not involve wholesale conversion of tissues to senescent states; it involves the gradual failure of clearance mechanisms to remove the small fraction of cells that do senesce.
| Context | Senescence type | Outcome |
|---|---|---|
| Embryonic development | Acute | Tissue patterning and organ formation |
| Wound healing | Acute | Fibroblast recruitment, then immune clearance |
| Aged lung tissue | Chronic | Low-level SASP, impaired repair capacity |
| Oncogene activation | OIS | Tumour suppression in pre-cancerous cells |
The SASP also illustrates how a single senescent cell can affect an entire tissue neighbourhood. One senescent cell secreting IL-6 and IL-8 can induce a paracrine senescence response in adjacent healthy cells, spreading the senescent phenotype without any new DNA damage. This “bystander effect” is one reason why even a small number of persistent senescent cells can have outsized consequences in aged tissue.
Cell-type variability in senescence has direct implications for cellular health and ageing. Skin fibroblasts, hepatocytes, and neurons each respond differently to the same stressor, and their SASP profiles differ accordingly. This variability is why researchers increasingly call for cell-type-specific senescence signatures rather than universal markers.
Key takeaways
Cellular senescence is a permanent, metabolically active cell state that serves both protective and pathological roles depending on whether immune clearance keeps pace with its generation.
| Point | Details |
|---|---|
| Definition and markers | Senescence is irreversible cell cycle arrest, identified by p16, p21, and SA-β-gal expression. |
| Two distinct types | Acute senescence is beneficial and transient; chronic senescence drives age-related disease. |
| SASP is the key mechanism | Senescent cells secrete pro-inflammatory factors that alter neighbouring tissue, for better or worse. |
| Senescent cells are rare in health | Only around 0.27% of alveolar type 2 lung cells are senescent, showing clearance normally works. |
| Senolytics are experimental | No clinically approved senolytic therapy exists; lack of specific markers remains the central barrier. |
Why I think we are asking the wrong question about senescent cells
The popular framing of senescence research is “how do we get rid of senescent cells?” That question is understandable, but it misses the more interesting problem. The real question is: why does the immune system stop clearing them efficiently?
Ageing, in this light, is not primarily a story of cells going wrong. It is a story of surveillance failing. The senescent cells were always being generated; what changes with age is the capacity to remove them promptly. This reframing has practical consequences. Therapies that target the immune environment may ultimately prove more durable than senolytics that target the senescent cell directly.
I have also noticed that health enthusiasts often treat senescence as uniformly bad, something to be eliminated. The embryogenesis and wound-healing data should give pause. A body with no senescent cells at all would be a body that cannot repair itself properly. The goal is not zero senescence. The goal is timely clearance and a well-regulated SASP.
For anyone interested in evidence-backed approaches to ageing, the honest position right now is that senolytic therapies are promising but unproven in humans. The biology is real. The clinical translation is not yet there. Scepticism and curiosity are both warranted.
— Jord
Vivetus and cellular health: what to read next
Cellular senescence sits at the heart of the science of healthy ageing, and understanding it is the first step toward making informed decisions about how you support your body over time.
Vivetus brings together scientifically grounded information and nutritional products aimed at supporting healthy ageing. Whether you are a researcher looking for a clear overview or a health enthusiast building a long-term approach to vitality, the Vivetus resource library covers the mechanisms behind ageing at the cellular level. Explore antioxidants and cellular ageing or browse the full range of age-supporting supplements at Vivetus to find products aligned with current ageing science.
FAQ
What is the simple definition of cellular senescence?
Cellular senescence is the permanent, irreversible arrest of cell division in response to stress, with the cell remaining metabolically active and secreting inflammatory signals known as SASP.
What causes cellular senescence?
The main causes are telomere shortening after repeated cell divisions, DNA damage, oxidative stress, and oncogene activation, all of which trigger p16 and p21 pathways to halt the cell cycle.
Are senescent cells always harmful?
No. Acute senescent cells support wound healing, embryogenesis, and tumour suppression; harm arises when chronic accumulation outpaces immune clearance.
How common are senescent cells in healthy tissue?
Senescent cells are rare in healthy tissue. Approximately 0.27% of alveolar type 2 lung cells are senescent in aged human lung, illustrating that normal ageing involves selective rather than widespread senescence.
Can senescent cells be removed therapeutically?
Senolytic drugs targeting senescent cells are under active investigation but remain experimental. The absence of specific, non-invasive human biomarkers is the primary barrier to clinical application.